
Being told you might need back surgery is a different kind of stress than ordinary back pain. The pain itself is bad enough – but the prospect of a discectomy or spinal fusion, with its recovery timeline, risks, and no guarantees of full relief, adds a layer of anxiety that makes the whole situation harder to navigate. What a lot of patients in Salt Lake and Utah Counties don’t know when they get that conversation with their surgeon is that non-surgical spinal decompression is a clinically supported option they haven’t yet tried – and that for many herniated disc and sciatica patients, it changes the outcome entirely.
This isn’t a dismissal of surgery. There are cases where it’s necessary and where delay creates real harm. But surgery for herniated discs and sciatica is frequently recommended before conservative options have been genuinely exhausted, and spinal decompression is one of the most effective of those options.
What Actually Happens to a Disc When It Herniates
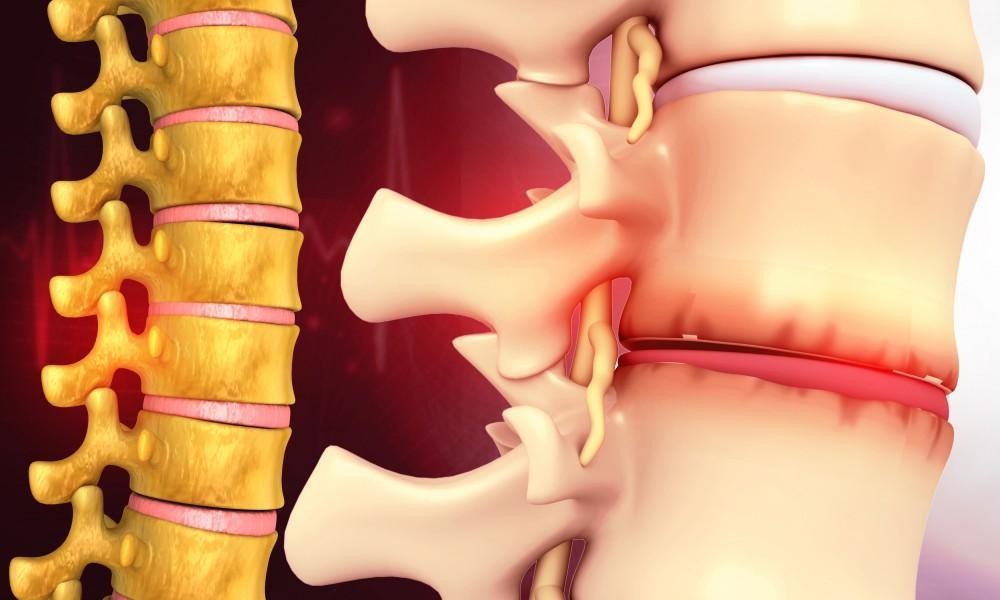
Understanding why decompression works starts with understanding what’s happening structurally when a disc herniates. Spinal discs are fibrocartilaginous structures that sit between each vertebra, acting as shock absorbers and allowing the spine to flex and rotate. Each disc has two main components: a tough outer ring called the annulus fibrosus and a gel-like interior called the nucleus pulposus.
Herniation happens when the nucleus pulposus pushes through a tear or weakness in the annulus – either partially, in what’s called a bulging disc, or fully, when the inner material ruptures through the outer layer. The problem isn’t just the tear itself. It’s what the displaced disc material touches. When a herniated disc pushes against a spinal nerve root, it triggers the pain, numbness, tingling, and weakness that characterize radiculopathy. When it’s the sciatic nerve being compressed, the result is sciatica – pain that can radiate from the lower back through the buttock and down the leg, sometimes as far as the foot.
The compression and the associated inflammation are what produce the symptoms. Remove the pressure, reduce the inflammation, and the nerve has a chance to recover. That’s the mechanical logic behind spinal decompression.
What the DRX9000 Does and Why the Mechanism Matters
Non-surgical spinal decompression at Draper Spinal Care uses the DRX9000 Lumbar True Spinal Decompression machine, a computer-controlled traction system that applies precise, variable pulling force to the lumbar spine. The distinction between the DRX9000 and older traction tables is significant and worth understanding.
Traditional traction applies a sustained pulling force that the body’s paraspinal muscles reflexively resist. When the muscles contract against the pull, the decompressive effect on the disc is largely negated. The DRX9000 uses a logarithmic pull pattern – the tension increases and decreases in cycles that are calibrated to stay below the threshold of the muscular guarding reflex. The muscles don’t fully activate in opposition, which means the decompressive force actually reaches the disc.
That decompression creates a negative intradiscal pressure – a reduction in pressure inside the disc itself. Two things follow from that. First, the disc material that has herniated or bulged is subject to a retraction force, drawing it back toward its proper position and away from the nerve it’s been compressing. Second, the negative pressure creates a fluid exchange effect, drawing in water, oxygen, and nutrients that the disc needs to heal but has limited access to because adult discs have poor direct blood supply.
Over a course of treatment – typically fifteen to thirty sessions depending on the severity and chronicity of the condition – this repeated decompression and fluid exchange can produce genuine structural change in the disc. The herniation reduces. The nerve has less compression. The pain pattern changes.
The Research Behind Spinal Decompression
Claims about disc retraction and nerve decompression are testable, and they have been tested. MRI studies comparing pre- and post-decompression imaging have documented measurable reduction in disc herniation size following a course of treatment with motorized decompression systems. A study published in the Journal of Neurological and Orthopaedic Medicine and Surgery found that a significant majority of patients with herniated lumbar discs reported substantial pain reduction following spinal decompression therapy, with outcomes sustained at follow-up.
Research published in Pain Physician has similarly supported non-surgical spinal decompression for discogenic low back pain and radiculopathy, with patient-reported outcomes showing meaningful improvement in pain and functional capacity.
It’s worth being precise about what this research shows and what it doesn’t. Spinal decompression is most strongly supported for discogenic conditions – herniated discs, bulging discs, degenerative disc disease with radiculopathy, and sciatica arising from lumbar disc pathology. It is not a treatment for all causes of back pain, and it is not appropriate for patients with certain contraindications including fracture, tumor, advanced osteoporosis, severe stenosis at the level being treated, or hardware from previous spinal surgery.
An honest evaluation of whether a patient is a candidate requires imaging review and a clinical examination – which is why Draper Spinal Care conducts a thorough consultation before recommending or initiating treatment.
What Surgery Involves and Why the Comparison Matters
Lumbar discectomy – the surgical removal of herniated disc material – is a well-established procedure with reasonable outcomes in properly selected patients. Spinal fusion, which joins two or more vertebrae to eliminate movement at a painful segment, is a more significant surgery with a longer recovery and a more complex risk profile.
Both procedures carry the standard surgical risks: infection, bleeding, anesthesia complications, and nerve injury. Fusion, specifically, introduces additional long-term considerations including adjacent segment disease – the accelerated degeneration of spinal segments above and below the fusion due to altered load distribution. Adjacent segment disease is not a rare complication. Studies report it occurring in a meaningful percentage of fusion patients within years of the procedure, sometimes requiring additional surgery.
None of that makes surgery wrong for patients who genuinely need it. A large, acute herniation that’s causing progressive neurological deficits – worsening leg weakness, loss of bowel or bladder function – is a situation where surgical consultation and likely intervention is appropriate and urgent. But for patients with chronic or subacute disc pain who’ve been told surgery might be an option rather than an emergency, the sequence matters. Conservative care tried first, surgery reserved for cases where it fails, is the approach most spine specialists now advocate.
Spinal decompression fits into that sequence as a conservative intervention with genuine structural mechanism and clinical support – not as a placeholder before the inevitable, but as a legitimate first-line approach for many patients whose imaging and presentation make them appropriate candidates.
What the Treatment Process Looks Like
Patients who come to Draper Spinal Care for spinal decompression start with a consultation that includes a review of any existing imaging and a clinical examination. If MRI or CT hasn’t been done recently, imaging may be recommended to confirm the diagnosis and rule out contraindications. Assuming the patient is a candidate, a treatment plan is developed with a defined number of sessions and a schedule that allows the disc to respond progressively.
Sessions on the DRX9000 typically run about thirty to forty-five minutes. The patient lies on the table, is secured with a pelvic harness, and the computer-controlled system cycles through the decompression protocol. Most patients find it comfortable – some report it as genuinely relaxing. There’s no recovery period afterward, and most patients return to normal activity the same day.
Progress is assessed through symptom tracking and, when appropriate, follow-up imaging. Patients whose herniation or bulge has produced significant nerve compression often notice changes in their symptom pattern – particularly a reduction in radiating leg symptoms – before the local back pain fully resolves, because the nerve compression is what’s been driving the referred symptoms.
Before You Agree to Surgery, Ask About Decompression
If you’ve been diagnosed with a herniated disc, bulging disc, degenerative disc disease with sciatica, or related lumbar condition and surgery has been presented as a likely next step, non-surgical spinal decompression is worth evaluating before you commit to anything more invasive.
Draper Spinal Care serves patients throughout Draper, South Jordan, Sandy, and the broader Salt Lake and Utah County areas. Call (801) 701-2111 to schedule a consultation and find out whether you’re a candidate for decompression treatment – and what it might realistically accomplish for your specific condition.